











Please select a partnership to see additional information:
1.17 Child Death Reviews
Under the Children Act 2004 there is a statutory requirement that all child deaths are independently reviewed.
The Child Death Review Statutory and Operational Guidance (England) (2018) sets out the key features of robust child death review and applies to all organisations involved with child death review processes.
The child death review process covers all children; a child is defined in the Children Act 1989 as a person under 18 years of age. A child death review must be carried out for all children regardless of the cause of death. This will include the death of any new-born baby (of any gestation) who shows signs of life following birth, or where the birth was unattended, but does not include those (of any gestation) who are stillborn where there was medical attendance, or planned terminations of pregnancy carried out within the law. The purpose of a child death review is to identify any matters relating to the death, or deaths, that are relevant to the welfare of children in the area or to public health and safety, and to consider whether action should be taken in relation to any matters identified. Where it is found that action should be taken by a person or organisation, they will be informed.
Contents
- Child Death Review Partners(Jump to)
- Responsibilities of other Organisations/Agencies(Jump to)
- Responding to the death of a child: the Child Death Review process (focus on the individual child)(Jump to)
- The independent review: Child Death Overview Panel (focus on local and national learning)(Jump to)
- National Child Mortality Database(Jump to)
The child death review partners are defined as the local authority for the relevant area and any integrated care boards operating in the local authority area as set out in the Children Act 2004 (the Act), as amended by the Children and Social Work Act 2017.
It is the responsibility of the Partners to ensure local processes are in place to provide a robust response to the review all deaths of children normally resident in the local authority area and, where it is considered appropriate, for any non-resident child who dies in the local authority area.
The Partners will publish information on the arrangements for child death reviews in their area on relevant websites.
In addition, the Partners will prepare and publish a joint annual report on:
- What they have done as a result of the child death review arrangements in their area; and
- How effective the arrangements have been in practice.
The Partners will request information from a person or organisation for the purposes of enabling or assisting the review and/or analysis process. Requests for information must be complied with and if they are not, the Partners will consider legal action to seek enforcement.
All local organisations or individual practitioners that have had involvement in the case will be required, as appropriate, to participate in the child death review process by the provision of written information (on the appropriate template) and attendance at meetings where discussions will take place about the child's death.
There are specific requirements on Registrars of births and deaths and on Coroners which are set out in the statutory guidance.
The process to be followed is set out in statutory guidance:
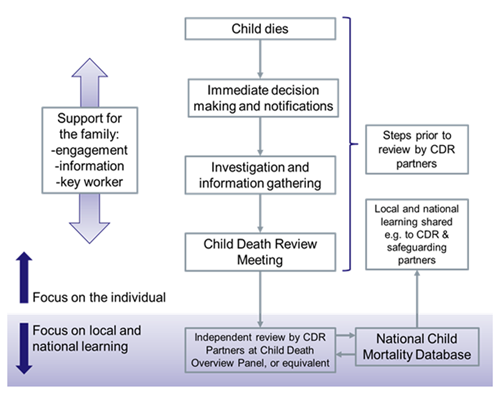
The steps that precede the independent review undertaken by the Child Death Overview Panel commence in the immediate aftermath of a child's death. These include the immediate decisions, notifications and parallel investigations, and the local case review, undertaken by those directly involved with the care of the child or in the investigation after death, at the Child Death Review Meeting (CDRM).
The functions of CDOP include:
- To collect and collate information about each child death, seeking relevant information from professionals and, where appropriate, family members;
- To analyse the information obtained, including the report from the Child Death Review Meeting (CDRM), in order to confirm or clarify the cause of death, to determine any contributory factors, and to identify learning arising from the child death review process that may prevent future child deaths;
- To make recommendations to all relevant organisations where actions have been identified which may prevent future child deaths or promote the health, safety and wellbeing of children;
- To notify the Child Safeguarding Practice Review Panel and local Safeguarding Partners when it suspects that a child may have been abused or neglected;
- To notify the Medical Examiner (once introduced) and the doctor who certified the cause of death, if it identifies any errors or deficiencies in an individual child's registered cause of death. Any correction to the child's cause of death would only be made following an application for a formal correction;
- To provide specified data to the National Child Mortality Database;
- To produce an annual report for CDR partners on local patterns and trends in child deaths, any lessons learnt and actions taken, and the effectiveness of the wider child death review process; and
- To contribute to local, regional and national initiatives to improve learning from child death reviews, including, where appropriate, approved research carried out within the requirements of data protection.
CDOPs will have a core representation (specified in the statutory guidance) and will include other professionals co-opted onto the Panel for specific individual cases or themed case reviews where they bring a particular expertise to the subject.
The key worker for the family should inform them of the CDOP meeting and its purpose. The family should be advised that it will not be possible to give case specific feedback.
From 1 April 2019 the National Child Mortality Database (NCMD) is the repository for data relating to all children's deaths in England. It will enable more detailed analysis and interpretation of all data arising from the child death review process, ensure that lessons are learned following a child's death and that learning is widely shared, and that actions are taken, locally and nationally, to reduce child mortality.